- Melanie Boeckmann1,
- Iveta Nohavova2,
- Omara Dogar3,
- Eva Kralikova2,
- Alexandra Pankova2,
- Kamila Zvolska2,
- Rumana Huque4,
- Razia Fatima5,
- Maryam Noor6,
- Helen Elsey7,
- Aziz Sheikh8,
- Kamran Siddiqi3,
- Daniel Kotz1,9 on behalf of the TB & Tobacco Project Consortium
- Correspondence to Dr Melanie Boeckmann; boeckmannmelanie@gmail.com
Abstract
Introduction Tuberculosis (TB) remains a significant public health problem in South Asia. Tobacco use increases the risks of TB infection and TB progression. The TB& Tobacco placebo-controlled randomised trial aims to (1) assess the effectiveness of the tobacco cessation medication cytisine versus placebo when combined with behavioural support and (2) implement tobacco cessation medication and behavioural support as part of general TB care in Bangladesh and Pakistan. This paper summarises the process and context evaluation protocol embedded in the effectiveness–implementation hybrid design.
Methods and analysis We are conducting a mixed-methods process and context evaluation informed by an intervention logic model that draws on the UK Medical Research Council’s Process Evaluation Guidance. Our approach includes quantitative and qualitative data collection on context, recruitment, reach, dose delivered, dose received and fidelity. Quantitative data include patient characteristics, reach of recruitment among eligible patients, routine trial data on dose delivered and dose received, and a COM-B (‘capability’, ‘opportunity’, ‘motivation’ and ‘behaviour’) questionnaire filled in by participating health workers. Qualitative data include semistructured interviews with TB health workers and patients, and with policy-makers at district and central levels in each country. Interviews will be analysed using the framework approach. The behavioural intervention delivery is audio recorded and assessed using a predefined fidelity coding index based on behavioural change technique taxonomy.
Ethics and dissemination The study complies with the guidelines of the Declaration of Helsinki. Ethics approval for the study and process evaluation was granted by the University of Leeds (qualitative components), University of York (trial data and fidelity assessment), Bangladesh Medical Research Council and Bangladesh Drug Administration (trial data and qualitative components) and Pakistan Medical Research Council (trial data and qualitative components). Results of this research will be disseminated through reports to stakeholders and peer-reviewed publications and conference presentations.
Trial registration number ISRCTN43811467; Pre-results.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Strengths and limitations of this study
-
Strengths of the process evaluation are its design by a multidisciplinary team, support from national tuberculosis programmes, and cultural and linguistic adaptations of the evaluation tools to the respective contexts.
-
Combining quantitative and qualitative data under the umbrella of the UK Medical Research Council process evaluation framework allows us to target the intervention components programme theory, implementation, mechanisms of impact and context.
-
Conducting the hybrid trial and implementation study under real-world circumstances alerts us to challenges and implementation barriers that can be addressed in intervention scale-up.
-
Potential limitations include the sensitivity of the tobacco use topic, the associated possible reluctance of participants to discuss their experiences and challenges of truly integrating the various data sources in the analysis.
Introduction
Tuberculosis (TB) is a widespread infectious disease caused by Mycobacterium tuberculosis, leading to an estimated 1.3 million deaths among HIV-negative persons and an estimated 10.4 million new TB cases in 2016.1 The majority of cases occur in Sub-Saharan Africa and South Asia.1 2 Pulmonary TB that affects the lungs is the most infectious form of TB, and tobacco use is a highly relevant risk factor for it.3 The WHO estimates that at least 20% of global TB incidence could be attributable to tobacco.4 Often referred to as ‘colliding epidemics’ of TB and tobacco use, 15% of the global pulmonary TB burden has been attributed to tobacco use.5 Tobacco use not only increases the risk of acquiring a TB infection, it also increases the risk of disease progression and worsens disease outcomes and mortality.3 6 Considering that in 2015, 1.1 billion people used a form of tobacco globally,7 and that low-income and middle-income countries (LMICs) have an increased disease burden attributable to tobacco consumption,8 it follows that tobacco cessation strategies delivered to patients with TB may contribute to reduced lung disease burden in these countries.
While studies from high income contexts have shown that tobacco cessation strategies combining pharmacological and behavioural support methods can be effective,9 10 such evidence is currently lacking for LMICs and for patients with TB in particular. Dedicated services to provide cessation support to tobacco users, and the infrastructure to support these services, do not often exist in LMICs.11 Provision of cessation services as a nationwide initiative is therefore not currently realistic in many of these countries. However, implementing tobacco cessation within existing TB care is both logical and potentially likely to benefit patients with TB over and above the general cessation benefits. In addition, few studies have investigated whether tobacco cessation concretely improves TB outcomes.12 The TB & Tobacco trial aims at filling this knowledge gap. Its main objectives are to investigate how tobacco cessation support can be integrated into national TB programmes using affordable cytisine, a low-cost pharmacotherapy, and to assess effectiveness of cytisine in these contexts.
TB & Tobacco trial
The 4-year project ‘Tobacco cessation within TB programs: A ‘real world’ solution for countries with dual burden of disease’ (TB & Tobacco) is a European Union Horizon 2020-funded study coordinated by the University of York and conducted together with eight international partners.i The project has two goals: first, to evaluate the effectiveness and cost-effectiveness of providing cytisine in addition to tobacco cessation behavioural support (effectiveness goal), and second to evaluate behavioural support implementation using process and context evaluation approaches (implementation goal). While the trial addresses the effectiveness goal, the intervention development phase, evaluations of process, context, sustainability and scale-up meet the implementation goal. Behavioural support for tobacco cessation will be implemented in routine TB care clinics at study sites in Bangladesh and Pakistan. The detailed trial protocol has been submitted for publication.
The trial compares active cytisine+behavioural support with placebo+behavioural support. Cytisine is a low-cost plant-derived alkaloid that mimics nicotine by targeting the same brain receptors.13 While cytisine has been proven an effective tobacco cessation medication in trials in Eastern Europe and New Zealand,13 14 there have not yet been any clinical trials in LMIC nor for patients with TB who could especially profit from quitting tobacco.6 Patients with TB who use tobacco will be randomly assigned to cytisine or placebo treatment. The multicountry and multisite trial has its primary outcome continuous abstinence at 6 months (self-reported), which is biochemically verified by a carbon monoxide level of <10 ppm and cotinine dip-stick level of <3 in urine (level 3=100–200 ng/mL cotinine) to detect smokeless tobacco use (effectiveness goal). Local partners are national non-governmental research organisations with extensive experience in tobacco control and the health systems in each country: The Initiative in Pakistan and ARK Foundation in Bangladesh. In Pakistan, additionally the National Tuberculosis Control Programme (NTP) is a principal investigator and leads planning and hospital-based implementation at respective trial sites. They will employ research assistants who will be stationed at the study sites during trial recruitment and follow-up.
The TB & Tobacco trial will be carried out in Bangladesh and Pakistan with the aim to implement tobacco cessation strategies (both behavioural support and cytisine) in standard national TB care. Seventeen sites in Bangladesh and 11 in Pakistan have been selected for participation in the trial based on the following criteria: geographical location within the country, TB patient care volume at health centre, care level (primary, secondary or tertiary), number of staff, conditions at location regarding work flows and willingness of centre leaders to participate in the study. Site locations vary from urban to rural regions, with a minimum new TB patient volume of 224 per month on average for 8 months for Pakistan and 91 for Bangladesh.
Trial recruitment is currently planned from July 2017 in Bangladesh and from June 2017 in Pakistan until March 2018, while behavioural support implementation is planned long term at activated sites in both countries from June 2017. Our process evaluation will conclude in April 2019.
Behavioural support intervention
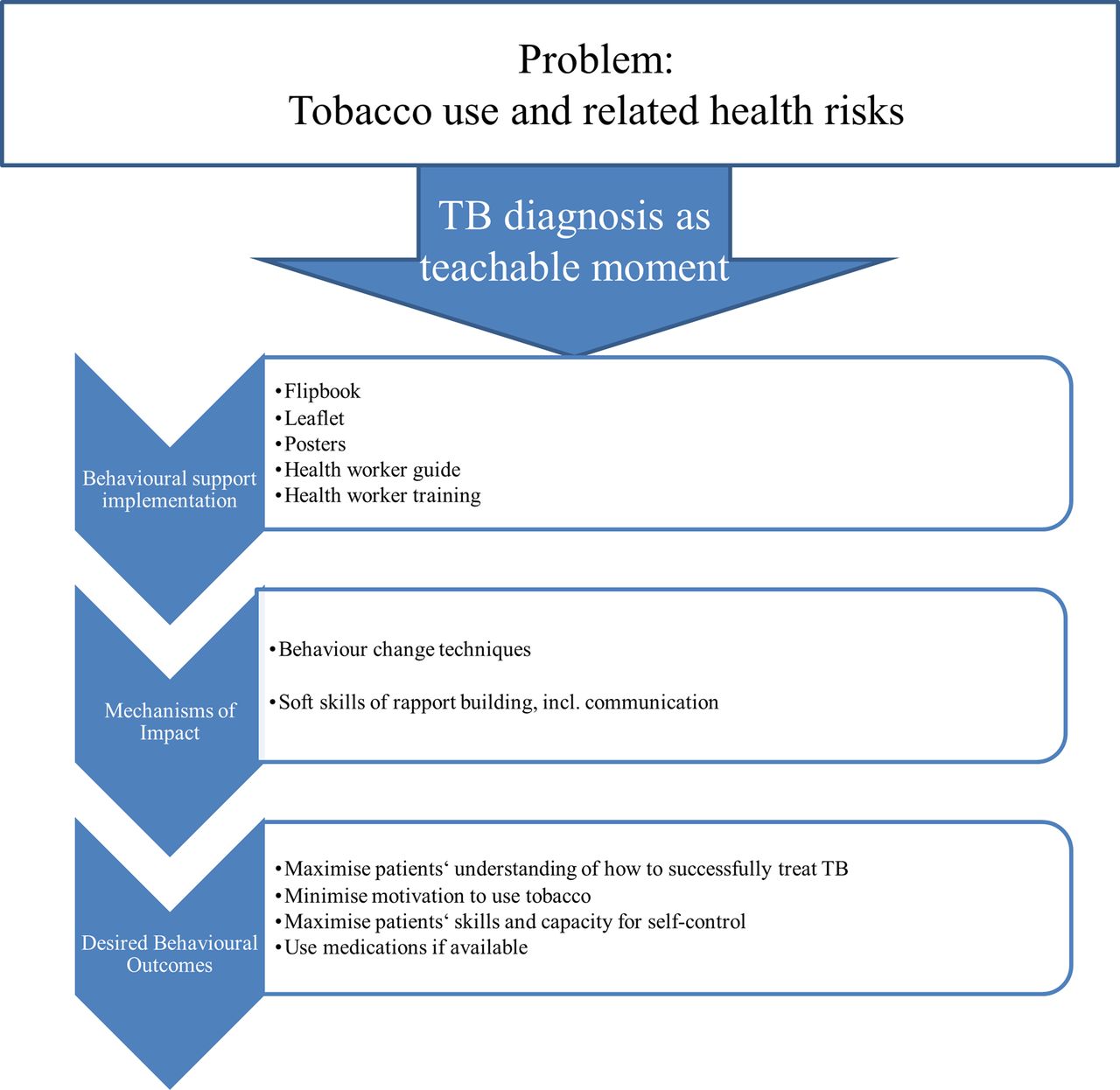
Phase I of the TB & Tobacco trial developed a brief behavioural support intervention. The intervention was based on previous work of the team testing the effectiveness of a behavioural support intervention in Pakistan15 and on feasibility testing of a similar intervention in primary care in Nepal.16 It includes behavioural change techniques (BCTs) found effective in tobacco cessation in high-income contexts,17 18 which were selected through a participatory ranking process during expert focus group discussions. A BCT taxonomy from a European context was chosen as no similar taxonomy has yet been developed for smoking cessation in lower income countries. The selected taxonomy has previously been used successfully in a stop-smoking trial for patients with TB in Pakistan, the action to stop smoking in suspected tuberculosis (ASSIST) trial.15 19 During phase I, national TB programme staff and people with TB in each of the countries provided feedback on the prototype intervention materials and processes through qualitative interviews and expert groups. Full details of the intervention materials development process, including the selected BCTs and messages, can be found in the project output report publicly available on the TB & Tobacco website.ii The intervention includes a flipbook containing key messages on managing TB and on how to quit tobacco use. These messages are delivered via photo images on the front of the slides and text for health workers on the back of slides and are reiterated in posters and leaflets. This type of flipbook is a familiar medium for health workers as these have previously been used in TB care, but had been lacking information on tobacco use. Similar materials have previously been used successfully in the ASSIST trial.15 One flipbook-based counselling session takes an estimated 15–20 min. The intervention is to be delivered once to all new TB tobacco users entering care at the study sites when they first receive counselling from a health worker, regardless of their subsequent participation in the trial.
The behavioural support intervention logic model is illustrated in figure 1. Health workers have a 2-day training to enable them to deliver the intervention. This training is interactive and focuses on the ‘soft skills’ of rapport building and communication skills to support health workers to use the materials and to provide BCT messages.

Figure 1
Logic model of the behavioural support intervention to quit tobacco. TB, tuberculosis.
Importance of the process evaluation within the TB & Tobacco project
While trial outcomes can give insights into effects of an intervention, effectiveness evaluations do not provide information on how an intervention could be reproduced or scaled up to additional level.20 Process evaluations embedded in trials help to systematically assess quality and delivery of an intervention, and to identify relationships between context, implementation and mechanisms of impact behind variations in outcomes.20 Systematic process evaluations ask the questions ‘Was the programme carried out as planned? And if not, how was it carried out?’ to avoid type III errors of evaluating effects of inadequately implemented interventions.21 For the TB & Tobacco project and its aim of sustainably integrating tobacco cessation into TB care, generating useful information for policy-makers regarding transferability of the intervention is of high importance.
Process evaluation objectives
Through assessing context, recruitment, reach, dose delivered, dose received and fidelity of the intervention, the process evaluation aims to:
-
systematically assess intervention implementation
-
identify mechanisms of impact between intervention and participants’ interactions with the intervention
-
assess the role of context in intervention implementation, impact, and intervention outcomes (table 1).22 23
Table 1
Process evaluation objectives, research questions and data sources
Methods and analysis
Process evaluation design and theory
The predefined TB & Tobacco process and context evaluation is a theory-based, multimethod evaluation guided predominantly by the UK Medical Research Council process evaluation framework.20 It is being conducted in addition to a randomised controlled trial which will establish cost-effectiveness of cytisine among patients with TB. Figure 2 illustrates how our process evaluation objectives and theories are linked to this framework. Within this overarching framework, the intervention programme theory based on BCTs17 informs causal assumptions of the intervention. Definition of implementation and its components for the purposes of this study is in line with Linnan and Steckler’s21 approach, and includes context, reach, dose delivered, dose received and fidelity. As fidelity, also called adherence to the intervention, and its interaction with adaptations to individual patient’s needs in the field is the subject of much debate,22 we will further subdivide fidelity into content, coverage, frequency and duration, as described.24 Fidelity will be assessed for adherence to intervention and for quality of delivery and further moderating effects of recruitment, context and participant responsiveness.25 See table 2 for data collection components sorted by clinical trial and behavioural support implementation.

Figure 2
Process evaluation framework (adapted from Moore et al 20). COACH, COntext Assessment for Community Health; COM-B, capability, opportunity, motivation and behaviour.
Table 2
Data collection components on behavioural support implementation and cytisine trial
Study participants
Behavioural support will be rolled out as standard care at the study sites in both countries. All adult tobacco users newly attending the study site clinics will be offered TB and tobacco cessation messages as part of their routine care, independently of their interest in or eligibility for the cytisine trial. Adult tobacco users diagnosed with pulmonary TB disease in the last 4 weeks and willing to quit tobacco, able to consent and to participate voluntarily are able to participate in the cytisine trial. Patients for whom research burden or study treatment can be expected to lead to adverse effects, and patients with contraindications for cytisine use will be excluded. Adults are defined according to national laws as being 15 years or older in Pakistan, and 18 years or older in Bangladesh. Participants for the interviews and fidelity assessment will also include those health workers who have agreed to be facilitators of the behavioural support intervention at their clinics.
Interview sampling at two case study sites per country
Aiming for in-depth understanding of the intervention process mechanisms, interviewing of patients and health workers takes place at two case study sites per country. These case study sites were preselected during a feasibility assessment. In Bangladesh, case study sites were selected to represent one typical urban and one typical rural site with sufficient administrative support for the process evaluation interviews. In Pakistan, case study sites represent one TB-specific hospital and one tertiary care hospital to investigate differences in implementation opportunities. The different sampling approaches for case study sites were chosen based on contextual health systems differences: in Pakistan diversity between clinics occurs owing to organisational type, whereas differences between urban and rural clinics characterise the Bangladesh system. All health workers providing TB counselling at case study sites will be invited to participate in the interview study and in the assessment of their experiences with the training provided as part of the intervention (n=2–4 per country). Health workers will be interviewed at three time points during the trial in Bangladesh and Pakistan to assess changes over time: once in fall 2017 shortly after trial start, once in winter 2017/2018 and once in spring 2018. The clinic in-charges (n=2 per country) at case study sites will be interviewed once after trial recruitment has ended in the Summer of 2018.
Among the patient collective, recruitment aims at capturing a range of experiences through a purposive and responsive strategy.26 Initial sampling for patient interviewing is based on key sociodemographic characteristics (eg, age, gender, education level, employment status and literacy level). The aim is to capture a range of voices by interviewing patients of different ages, education levels, employment status and literacy level throughout the study. Ideally, 10 patients per case study site (n=20 per country) will consent to be interviewed twice, once immediately after receiving the behavioural support (up to 5 days after their first clinic visit) and once a few weeks later. A purposefully selected sample of TB experts among policy-makers at national (n=2 per country) and district level (n=2 per country) will be interviewed once in each country.
Data collection
A wide range of data sources will be used to generate understanding of the TB & Tobacco intervention and its delivery and implementation. Our process evaluation uses a mixed-methods approach to collect quantitative and qualitative data on all three evaluation objectives. Data will only be collected from consenting participants adhering to confidentiality and ethical practice specified in the ethics approval.
Data sources for objective 1: to systematically assess intervention implementation
Our implementation evaluation targets the questions of actual versus planned intervention delivery and of barriers and facilitators to delivery as planned. The assessment will include the following intervention components: recruitment, reach, dose received, dose delivered and fidelity.
Characteristics of eligible and included or non-included patients
For a comparison of eligible/included versus eligible/not included tobacco users, individual, but non-identifiable routine TB patient data from TB programmes of the selected study sites will be extracted from TB registers, screening logs and eligibility forms. This includes age and sex, and TB-related data such as pulmonary or extra pulmonary diagnosis, smear positive or smear negative test, new treatment or retreatment phase.
Reach
Routine patient data extracted from Trial Case Report Forms by local research assistants for the patient characteristic assessment will be used to calculate the proportion of included participants among all eligible patients for each month of the recruitment phase.
Dose delivered and dose received
Non-identifiable routine data from the trial dataset on study medicine and behavioural support delivered to patients will be extracted from the trial database.
Semi-structured interviews with health workers participating in the study at the case study sites in both countries will cover aspects of tobacco use context, implementation and mechanisms. Context-related questions include tobacco use rules at work places and the TB clinic, tobacco availability near the clinic and health worker routines that might be disrupted by delivering behavioural support. Topics relating to implementation and mechanisms of impact include acceptability and perceived effectiveness of the behavioural support and key BCTs, barriers and facilitators to the implementation of the behavioural support, perceived use of trainings, perceived compatibility of general TB messages and specific tobacco cessation messages and health workers’ suggestions for implementation beyond the trial (see interview guide template in English in online supplementary file 1).
Supplementary file 1
Patient interviews will be semi-structured as well and conducted in a purposive sample of patients (see section on Interview sampling at case study sites for criteria). Interview guides cover contextual, implementation and interaction aspects. For context, information will be generated on, among others, tobacco habits among families and friends, tobacco rules at patients’ work places, burden of TB medication and tobacco cessation regimens, social support for quitting tobacco and tobacco availability near the clinic and patients’ houses and work place. Topical interview guides further address patients’ experience with the received behavioural support and specific BCTs, contextual factors, perceived usefulness of the leaflet, impressions of the TB health in context with tobacco cessation messages and patients’ relationship to practitioner. Regarding mechanisms of impact, interview guides include questions on patients’ and health workers’ impressions on intervention effectiveness, possible changes to tobacco use culture among their social network, necessary adaptations to the programme, recommendations for future programme iterations and consequences of receiving or providing tobacco cessation will be elicited.
A sample of three to five behavioural support sessions from all study sites will be audio recorded with consent, and coded for intervention content, coverage, frequency and duration using a standardised fidelity coding index predeveloped specifically for the TB & Tobacco behavioural support intervention. Both early and later stages of the intervention will be included to observe a range of delivered session, and to identify learning effects or reasons for deviations from the intervention scripts. The fidelity coding index draws from previous similar work on quantitative measurement of fidelity19 and incorporates BCT contents as well as delivery quality.27 Coding will be done by a group of bilingual researchers and cross-checked by the process evaluation team. The analysis of fidelity data will include the: (1) description of intervention fidelity by providers as assessed by implementing the fidelity index, (2) association between intervention fidelity and patient quit rates and (3) mediation and moderation pathways for adherence to intervention content and quality of delivery. All analyses will be conducted by at least two researchers using SPSS,28 SAS29 or R,30 depending on the institute.
Data sources for objective 2: to identify mechanisms of impact between intervention and participants’ interactions with the intervention
Reasons for non-participation
Health workers delivering the behavioural support will record at regular intervals the reasons given by patients refusing to set a tobacco quit date as part of their counselling session. Patients’ names or any other identifying information will not be included in the information collected. Local research assistants will collect these sheets from all sites in each country, translate into English and share with European research partners for analysis of behavioural support implementation.
Anonymised data on non-participation in the trial in Bangladesh and Pakistan will be extracted from the patient eligibility screening forms that are part of routine trial data.
Interviews with health workers and patients
Interview topic guides and interview procedures for mechanisms of impacts are included in the implementation assessment described above.
Data sources for objective 3: to assess the role of context in intervention implementation, impact and intervention outcomes
Context in this study is described as factors that can either positively or negatively influence the delivery of tobacco cessation strategies in healthcare settings. The overall aim of the contextual evaluation is to understand the influence of those factors that are considered beyond the control of the healthcare professionals, the intervention and the patients, but could nonetheless potentially influence the outcomes under study.31
TB health workers’ competences and motivation to deliver tobacco cessation
The COACH (COntext Assessment for Community Health) and COM-B (‘capability’, ‘opportunity’, ‘motivation’ and ‘behaviour’) questionnaires32 33 were adapted to the Bangladeshi and Pakistani contexts and pretested, and will be administered to all health workers at all study sites at a minimum of three time points during the study: shortly after the implementation of the behavioural support package starts, at midpoint and at endpoint of the study. The COM-B scale will be completed by all health workers caring for patients with TB in the study sites at the three time points, as well as before and after any training. The COACH questionnaire will be completed by the facility managers/in-charges at each study site. These questionnaires will provide an overview of knowledge, skills, attitudes and opinions of healthcare workers over the course of the study and allow for assessment of changes occurring over this period.
Guided observation and survey on environmental and social aspects of tobacco use
Local research assistants stationed at or near study sites in Bangladesh and Pakistan will be asked to fill in guided observation portfolios for each site. These will include field notes on access to study location, environmental noise, availability and privacy of counselling rooms, state of waiting areas, tobacco availability near clinics and similar items relevant to intervention delivery. Photos of infrastructure complete these observation portfolios.
A structured, written survey to be filled in by the research assistants for each site contains questions on tobacco regulations at the participating TB clinics, perceived support within clinics for tobacco cessation, tobacco use at facilities, perceived barriers and facilitators for intervention delivery (see online supplementary file 2 for the observation template).
Supplementary file 2
Research assistant updates
To better understand routine or infrastructural changes that may occur during the project, research assistants stationed at or near study sites will be asked to update research teams regularly on uncommon or unexpected occurrences. These data will be consulted during interpretation of interview data.
Interviews
All interviews conducted with health workers and patients for implementation assessment also cover context-related questions as described above. In each of the two countries, approximately five additional semi-structured interviews will be conducted to understand health service context and opportunities for scale-up of the intervention: one with central level staff of the NTP, two with district level NTP staff and two with the case study sites facility managers/in-charges. Interview guides include financial and other resources allocated to tobacco cessation, TB care infrastructures, perceived challenges for patients with TB to quit tobacco, as well as for TB health workers to provide tobacco cessation.
Data analysis
Quantitative data
All quantitative data will be securely stored as electronic files, including anonymised routine trial data, questionnaires, anonymised routine patient data and research assistant surveys. Characteristics of eligible and included or non-included patients, reach, cytisine dose delivered and dose received data from the trial database will be analysed using descriptive statistics and correlation analyses. Results will be reported stratified by gender and additional demographic characteristics where possible. COM-B and COACH questionnaires will be analysed using descriptive statistics: frequencies of items, statistical dependence analysis and correlation analysis. Research assistant surveys will be analysed quantitatively using descriptive statistics for frequencies of statements regarding no smoking regulations at clinics and qualitatively using thematic analysis on the free text answers on site conditions and behavioural support processes observed by the research assistants.
Qualitative data
All qualitative data will be securely stored as written electronic files, including interview transcripts, observation memos, research assistant update notes and non-participation descriptions. Data collection and analysis will occur concurrently in line with qualitative research quality guidelines.34 Interviews with health workers, patients, and policy-makers will be audio recorded with consent, transcribed verbatim, translated into English and jointly analysed by local teams and the process evaluation team using NVivo Pro V.11 software.35 Before analysis, all transcripts will be pseudonymised. Interviewers will write field notes after interviews to generate contextual knowledge and support interpretation of interview data. Observations on site access and surroundings as part of the research assistant observation will be included in the qualitative analyses.
Interview analyses
Using a combined deductive and inductive approach, a predefined coding framework based on constructs outlined in the Consolidated Framework for Intervention Research (CFIR)36 37 and in the Theoretical Domains Framework (TDF)38 39 will be used in data analysis while allowing for new codes on emerging issues.
CFIR has been proposed as an analysis framework suitable for complex interventions as well as for lower-income settings.40 The CFIR outlines ‘a comprehensive taxonomy of operationally defined constructs from multiple disciplinary domains (eg, psychology, sociology, organizational change) that are likely to influence implementation of complex programs’ (36:2). CFIR is particularly interested in those factors that influence implementation success and consists of five domains: intervention characteristics, outer setting, inner setting, characteristics of individuals and process.37 However, since the behavioural support intervention in the TB & Tobacco project is built on BCTs,18 41 the CFIR alone is unlikely to capture the processes related to specific tobacco cessation behaviours advocated by the intervention. To assess these aspects, TDF that builds on the same BCT theories38 39 as used in intervention development will be employed and combined with CFIR for a tailored framework approach.42
All results will be reported stratified by gender and additional sociodemographic characteristics where possible.
Triangulation and data synthesis
As both qualitative and quantitative data are collected concurrently throughout the project data collection period, constant comparative iterative analysis allows for thorough integration of the individual data sources and findings.43 44 In practice, this means all collected data will be compared and contrasted to see whether contradictions between data sources can be observed, or whether data from interviews can help make sense of observed implementation practice in the audio recordings or the quantitative routine data. The aim of such triangulation is to become aware of issues that were not anticipated, and to validate findings by looking for similarities across data sources.
Our process evaluation is not formative for immediate changes to the programme unless ethical issues require such immediate adaptations, but early findings will be reported to the project teams and may be considered in the design and implementation of sustainability and scale-up strategies after the trial.
Ethics and dissemination
Tobacco use can be associated with stigma and might be a sensitive topic among the study target group. Gender, level of literacy and/or social status may influence the willingness of patients and health workers to engage on the topic of tobacco use. The research team is aware of these issues and will tailor the conversations accordingly, for example, through building rapport with patients before broaching the topic of tobacco. All data collection will be preceded by participants’ written informed consent. Quantitative data will be collected by local research assistants at trial sites, anonymised and uploaded to the main trial database, from which the process evaluation team will extract only unidentifiable patient data. Patients will give consent to the use of their data as part of the overall trial consent procedure.
Interview and fidelity data require additional written consent, without which interviews or fidelity recordings will not be conducted. Provided consent forms are adaptable for illiterate patients and allow for signature by thumbprints, an approved and widespread procedure in the study countries.45–47 Interview transcripts will be pseudonymised before analysis. All participants will be informed that they may withdraw from the study at any time without compromising their regular care at the TB clinics.
The study complies with the guidelines of the Declaration of Helsinki. Results of this research are expected to be disseminated through reports for stakeholders and via scientific forums, specifically peer-reviewed publications and conference presentations in 2018 and 2019.
Acknowledgments
The authors thank the organisations and people participating in the trial, especially the health workers, patients and policy-makers generously giving their time and insights in the data collection phase. Special thanks go to the National TB Programs in the two countries and their representatives for facilitating the study. Many thanks to the in-country teams conducting the process evaluation: for Pakistan, Maryam Noor, Dr Raana Zahid and Dr Amina Khan; for Bangladesh, Dr Rumana Huque, Dr Deepa Barua, Esha Haowa Mustagfira and their respective teams, without whom no data could be collected or analysed. The authors also thank the TB & Tobacco project manager Dr Anne Readshaw as well as the TB & Tobacco Consortium. TB & Tobacco is coordinated by the University of York.
Footnotes
-
↵i https://www.york.ac.uk/healthsciences/research/public-health/projects/tb-tobacco/
-
↵ii https://www.york.ac.uk/healthsciences/research/public-health/projects/tb-tobacco/achievements/.
-
Contributors DK leads the design of the process evaluation; EK leads the design of the context evaluation. MB and DK jointly developed the process evaluation protocol, designed the quantitative and qualitative process evaluation data collection and analysis strategies, and cowrote the manuscript. MB and IN conduct the process evaluation together with RH, MN and local teams. OD is the TB & Tobacco trial coordinator and contributed to the quantitative data collection tool development, codeveloped the fidelity coding index and contributed to the writing of the manuscript. IN, EK, AP and KZ designed the context data collection tools and context data analysis strategies and contributed to the writing of the manuscript. RH leads trial implementation in Bangladesh, contributed to the design of the process evaluation strategy and to the writing of the manuscript. RF leads the implementation into routine care at NTP Pakistan and contributed to the writing of the manuscript. MN contributed to the design of the process evaluation, the data collection tools and to the writing of the manuscript. HE developed the behavioural support package implemented in the study and contributed to the process evaluation framework development, the design of the qualitative data collection tools and analysis approach and to the writing of the manuscript. AS contributed to the trial development and to the writing of the manuscript. KS and the TB & Tobacco team conceived of the trial. KS contributed to the process evaluation framework development and to the writing of the manuscript. All named authors contributed to the manuscript and agreed on its final version.
-
Funding This work was supported by the European Union’s Horizon 2020 research and innovation programme under grant agreement no 680995. Aflofarm Pharma Poland provides cytisine and placebo for the trial free of charge.
-
Disclaimer This publication reflects merely the authors’ views, and the European Commission is not responsible for any use that may be made of the information it contains. The funding agency had no role in designing or conducting the study, or in preparing this manuscript.
-
Competing interests EK, KZ and AP received payment for clinical studies and educational activities from Pfizer. They received no funding from a cytisine producing pharmaceutical company. KS received a research grant from Pfizer (2015–2017) to study the effect of varenicline (a smoking cessation medicine) on waterpipe smoking cessation.
-
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
-
Ethics approval University of Leeds (qualitative components), University of York (trial data and fidelity assessment), Bangladesh Medical Research Council and Bangladesh Drug Administration (trial data and qualitative components), Pakistan Medical Research Council.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Interview data are available to researchers on reasonable request.
-
Collaborators TB & Tobacco Consortium.

{kind=link}
{kind=link}